Safety must always come first, and so is also the case when carrying or babywearing. But what aspects do you need to consider? Is it the same for every one? Is something more important than others?
In my point of view, as a carrying consultant and as a NICU/Neonatal nurse, one triumphs them all: keeping the airways free and secure. Here’s why!
So, first and foremost, children are not just smaller adults. In the case of airways there’s a few crucial differences:
– softer trachea (that is the windpipe)
– larger head in proportion to their body (especially the back of the head)
– depending on age, their ability to change position and/or communicate may be limited
– children’s cardiac arrests usually comes from respiratory causes (begins with hypoxia leading to bradycardia and eventually a full cardiac arrest). This is why pediatric and neonatal CPR is so focused on adequate ventilation.
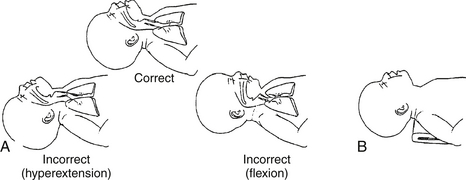
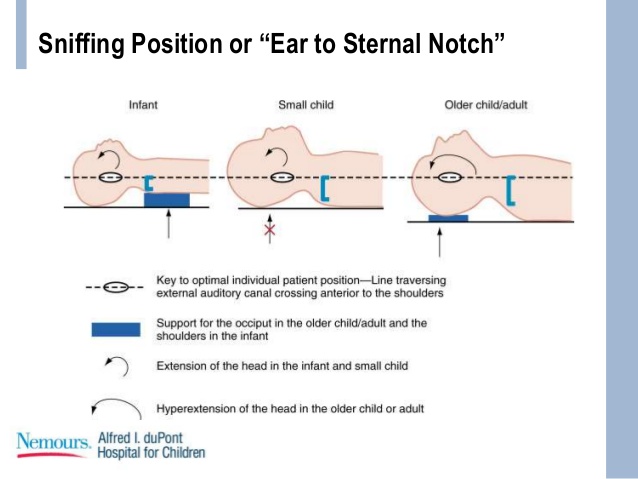
Many refer to the “sniffing position” which is a great tool for airway management. Putting someone in the sniffing position is a way of getting a clear and straight line from the back of the mouth down to the vocal cords (the position can help massively in cases of intubation), and achieving a nice free airway. But with children the angle in which the neck is tilted and flexed needs some attention, since an hyperextension (and a too big angle of tilt) as well as an flexion towards the child’s chest (and a too small angle of flexion) may BOTH cause blocked airways due to the anatomy of children.
This is an illustration of a newborn child where a sniffing position/free airway is achieved by placing a folded towel (or similar object) under the infants shoulders.
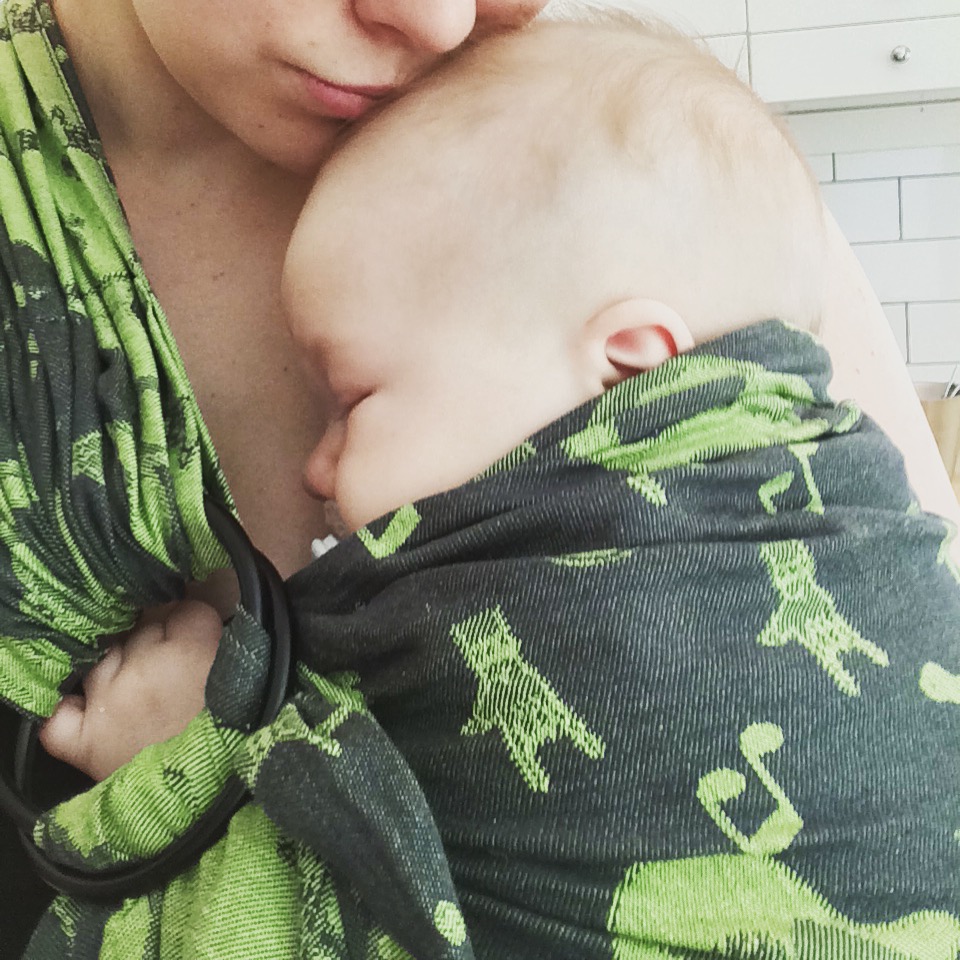
So, why does this matter in carrying? Because there is a risk of a compromised airway if the baby’s chin would fall forward towards the baby’s own chest or if the baby’s face would be pressed up against the carrier or the adults body. And as stated before cardiac arrests in infants usually generally begins with hypoxia. And it has happened before and the other week it happened again… I write this post, knowing that it might frighten some parents and scare them of from carrying which is far from my intention but no family should have to go through an experience like the loss of a child due to an avoidable situation. This is WHY we have all kinds of abbreviations to keep carried babies safe, such as TICKS, the circle of safety and ABC. These guidelines are not just for infants or front carries, but should be considered all the time, for everyone and all carries.

I would also like to mention the fit of a carrier, and the ways one might be encouraged to adapt or modify carriers to fit a smaller baby, if you do not have the option to buy or trade to another carrier do not hesitate to reach out to a trained consultant or peer supporter to get professional help and assistance in modifying your carrier in a safe manor.
So, in other words: CARRY ON & CARRY SAFE!